Table of Contents >> Show >> Hide
- What the 2018 Nobel Prize Actually Recognized
- Why James P. Allison’s CTLA-4 Discovery Changed Everything
- How Cancer Immunotherapy Changed the Treatment Landscape
- The Promise Came With Real Limits
- Why the Nobel Prize Mattered Beyond the Medal
- Experiences Shaped by the Immunotherapy Revolution
- Conclusion
- SEO Metadata
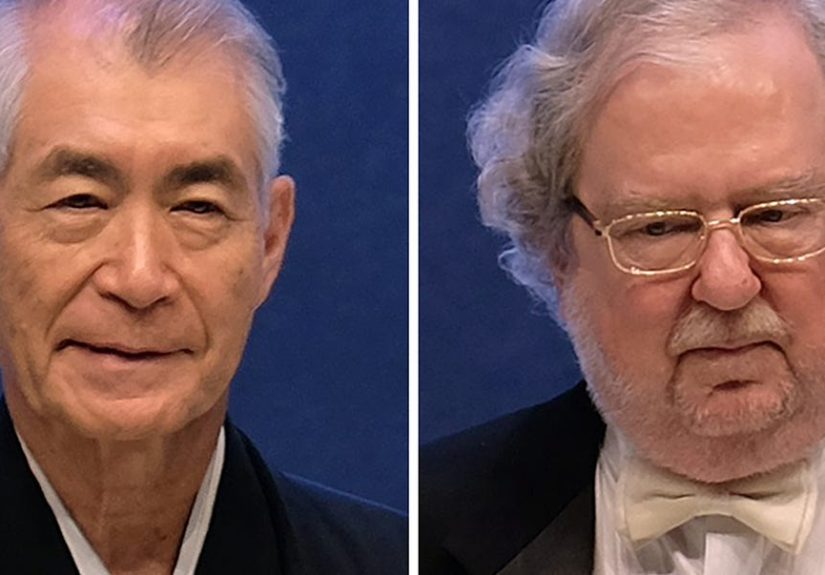
Some scientific breakthroughs arrive with fireworks. Others arrive wearing a lab coat, carrying years of stubborn data, and quietly changing medicine forever. The 2018 Nobel Prize in Physiology or Medicine belonged in the second category. It honored James P. Allison and Tasuku Honjo for discoveries that helped turn cancer immunotherapy from a fascinating idea into a treatment strategy that could genuinely change lives.
For James P. Allison in particular, the recognition was a victory for a bold scientific hunch: instead of attacking cancer cells directly, why not help the immune system do its job better? That sounds obvious now, but for decades cancer treatment mostly focused on surgery, radiation, and chemotherapy. Allison’s work helped open a different door. He showed that a molecule called CTLA-4 acts like a brake on T cells, and that blocking that brake could unleash an anti-tumor immune response.
That idea did not merely add a fresh chapter to oncology. It rewrote the table of contents. Suddenly, the immune system was not just supporting cast. It was the lead actor, the stunt double, and occasionally the entire plot twist. The 2018 Nobel Prize in Medicine mattered because it recognized a scientific revolution already reshaping how doctors think about melanoma, lung cancer, kidney cancer, bladder cancer, and other malignancies. More importantly, it recognized the kind of research that starts in basic immunology and ends at the bedside, where patients care a lot less about elegant diagrams and a lot more about whether a treatment gives them more time.
What the 2018 Nobel Prize Actually Recognized
The Nobel Prize in Medicine 2018 was awarded jointly to James P. Allison and Tasuku Honjo for their discovery of cancer therapy by inhibition of negative immune regulation. That official phrase is accurate, but it is not exactly party conversation material. In plain English, the prize celebrated the discovery that the immune system has built-in “off switches,” and that cancers can exploit those switches to avoid being destroyed.
Allison’s contribution centered on CTLA-4, an immune checkpoint that restrains T-cell activation. His work showed that CTLA-4 does not help the immune system attack tumors. It helps hold the immune system back. Once Allison and colleagues demonstrated that blocking CTLA-4 could trigger anti-cancer activity, the field of immune checkpoint blockade began to take shape.
Honjo’s work on PD-1 revealed another immune brake that works differently from CTLA-4 but can also be manipulated therapeutically. Together, these discoveries gave oncologists a new playbook: instead of trying only to poison or cut out cancer, remove the molecular disguises and restraints that keep immune cells from doing their work.
The Nobel committee’s choice was not a ceremonial pat on the back for an interesting lab concept. It was recognition that cancer immunotherapy had become one of the most important advances in modern medicine. The prize honored the science, yes, but it also honored the enormous shift in clinical thinking that followed.
Why James P. Allison’s CTLA-4 Discovery Changed Everything
To understand Allison’s impact, it helps to picture the immune system as a car built by engineers who were deeply worried about lawsuits. It has an engine, plenty of horsepower, and several emergency shutoff systems. That makes sense. An immune system with no brakes would attack normal tissue and cause dangerous autoimmunity. The problem is that cancer, being annoyingly resourceful, can benefit from those brakes.
Allison discovered that CTLA-4 functions as one of those braking systems on T cells. Rather than stimulating an immune attack, CTLA-4 dampens it. His insight was simple but radical: if CTLA-4 is holding T cells back, maybe blocking CTLA-4 could free them to attack cancer.
That hypothesis was not universally embraced at first. Cancer research has a long history of promising ideas that looked wonderful in mice and far less wonderful in humans. But Allison kept pushing. Preclinical work showed that antibodies blocking CTLA-4 could lead to tumor rejection in animal models. That finding cracked open a new therapeutic strategy: do not just target the tumor; target the immune regulation that protects the tumor.
The clinical payoff arrived with ipilimumab, an anti-CTLA-4 antibody. In 2011, the U.S. Food and Drug Administration approved ipilimumab for unresectable or metastatic melanoma, making it the first checkpoint inhibitor approved by the FDA. That was a landmark moment. Before then, advanced melanoma had a grim reputation and limited effective treatment options. Ipilimumab did not help every patient, but it proved something bigger than a single drug result: checkpoint blockade could produce meaningful and sometimes durable benefit in human cancer.
That is why Allison’s work matters so much in the history of oncology. He did not simply help develop one therapy. He helped establish a whole treatment philosophy. Once researchers saw that one checkpoint could be blocked successfully, the search accelerated for others. That momentum led to therapies targeting PD-1 and PD-L1, as well as new checkpoint strategies still being explored today.
How Cancer Immunotherapy Changed the Treatment Landscape
The phrase unleashing the immune system gets used a lot in articles about immunotherapy, and for once the cliché actually earns its paycheck. Checkpoint inhibitors work differently from chemotherapy. Chemotherapy attacks rapidly dividing cells directly, which is why it can also damage healthy tissues like hair follicles and the lining of the gut. Checkpoint inhibitors, by contrast, help immune cells recognize and attack cancer more effectively.
That difference matters because it created a new category of possibility. In some patients, immune checkpoint inhibitors have produced long-lasting responses that changed expectations about survival. Melanoma became the early proof point, but the impact did not stay there. Today, checkpoint inhibitors are used across a wide range of cancers, including lung cancer, kidney cancer, bladder cancer, head and neck cancer, certain colorectal cancers, liver cancer, and more.
Allison’s CTLA-4 work was especially important because it showed that the immune system’s regulatory pathways were not just biological trivia. They were drug targets. Once that became clear, immunotherapy moved from speculative science to frontline medicine. Researchers and clinicians began to think more strategically about combinations, biomarkers, sequencing, resistance, and how to extend responses across tumor types.
That also changed the culture of cancer care. Immunotherapy encouraged a more dynamic view of treatment response. Tumors do not always behave neatly under checkpoint blockade. Some patients may not show an immediate dramatic shrinkage. Others may experience unusual response patterns that require careful interpretation. Oncology had to adapt, and so did patients and families learning that the path of response in immunotherapy can look different from the classic chemo story.
And yes, this is the part where science gets a little cinematic. Instead of sending in chemical wrecking balls, medicine began learning how to remove the “Do Not Disturb” sign from cancer cells and let the body’s own defenses get loud.
The Promise Came With Real Limits
As transformative as checkpoint inhibitors have been, they are not magic. They do not work for every patient, every tumor, or every stage of disease. Some cancers are more visible to the immune system than others. Some tumors build highly suppressive microenvironments. Some patients respond beautifully at first and later develop resistance. Others never respond at all.
That reality is one reason the 2018 Nobel Prize in Medicine was so important. It recognized a major scientific foundation, not the final answer to cancer. Allison’s work launched a revolution, but revolutions are messy. They create new questions as fast as they solve old ones.
Then there are the side effects. Because checkpoint inhibitors remove immune restraints, they can also cause the immune system to attack healthy tissues. Common side effects can include rash, diarrhea, and fatigue. More serious immune-related adverse events may involve inflammation of the lungs, liver, colon, endocrine glands, skin, kidneys, or other organs. CTLA-4 blockade in particular has long been associated with a higher burden of certain immune toxicities compared with some PD-1 or PD-L1 strategies.
That tradeoff is the central tension of modern immunotherapy: the very thing that makes the treatment powerful can also make it unpredictable. Doctors need to monitor patients closely, and patients need to report symptoms early. A small rash or mild diarrhea can be just a nuisance, or it can be the opening scene of a much bigger plotline. Oncology teams have had to develop expertise not only in giving these drugs, but in managing the immune complications they can trigger.
Why the Nobel Prize Mattered Beyond the Medal
Nobel Prizes do not treat patients, but they do shape scientific attention. When the 2018 prize went to Allison and Honjo, it sent a global signal that immunotherapy had moved from promising frontier science to a defining achievement in medicine. That mattered for researchers, institutions, funders, and future clinicians.
It also highlighted a truth that science sometimes struggles to market well: basic research saves lives. Allison was studying T-cell biology and immune regulation, not building a quick-fix gadget for a flashy product launch. The path from CTLA-4 discovery to Nobel Prize to checkpoint inhibitor therapy took years of work, skepticism, refinement, and clinical testing. That is how major medical progress often happens. Slowly. Unevenly. With enough setbacks to make a less stubborn scientist go learn golf.
The award also helped the public understand why James P. Allison’s work in cancer immunotherapy was so influential. He did not discover “the cure for cancer,” a phrase that tends to flatten science into nonsense. He helped reveal a principle that changed treatment for many cancers and opened countless new research avenues. That is more realistic, more useful, and honestly more impressive.
In medicine, the biggest breakthroughs are often the ones that change what questions people ask next. Allison’s work did exactly that. It pushed researchers to ask which patients are most likely to benefit, how therapies can be combined, how resistance develops, and how new checkpoints can be targeted. The field is still answering those questions.
Experiences Shaped by the Immunotherapy Revolution
One reason the story of the 2018 Nobel Prize continues to resonate is that it is not just a laboratory success story. It is also a story of lived experience. In clinics, infusion centers, hospital rooms, research meetings, and family kitchens, cancer immunotherapy changed what people talk about when they talk about hope.
For oncologists, checkpoint blockade introduced a different kind of conversation with patients. Instead of saying, “We are going to hit the tumor directly,” doctors could explain that the treatment was designed to help the immune system do the hitting. That changes expectations. It changes how scans are interpreted. It changes how side effects are monitored. It even changes the emotional rhythm of treatment, because immunotherapy responses can be delayed, dramatic, incomplete, or surprisingly durable.
For patients, the experience can feel both encouraging and confusing. On one hand, hearing that the body’s own immune system can be recruited against cancer is powerful. It sounds more elegant than carpet-bombing cells with toxic chemicals, and sometimes it is. On the other hand, immunotherapy can come with its own brand of uncertainty. A patient may feel well and still be anxiously waiting for imaging results. Another may have a tumor response but struggle with fatigue, rash, colitis, or endocrine problems that require steroids and long-term follow-up. Hope and vigilance often travel together.
For researchers, Allison’s Nobel-winning work validated decades of persistence. Many scientists in immunology know the experience of working on a pathway that seems obscure until, suddenly, it is not obscure at all. CTLA-4 was once the kind of molecular detail that lived comfortably in specialist journals and conference slides. After checkpoint blockade proved clinically useful, it became part of the vocabulary of modern oncology. That shift is thrilling, but it also raises the bar. Once a field becomes clinically relevant, every unanswered question feels more urgent because real patients are waiting on the other end of the science.
Families have their own version of the experience. Immunotherapy often introduces a new language into the household: T cells, biomarkers, PD-1, inflammation, autoimmune toxicity, progression, remission. Loved ones learn to celebrate small victories and respect strange symptoms. A new cough is not always “just a cough.” A bout of diarrhea may not be food-related. A skin rash may be minor, or it may signal immune activation that deserves quick medical attention. In that sense, cancer immunotherapy is not only a treatment. It is an education.
There is also a broader emotional experience attached to this Nobel story. The prize reminded people that modern medicine still makes giant leaps. Not every advance is incremental. Sometimes a researcher asks a question that changes the treatment map for an entire disease category. That is what happened with James P. Allison’s work in cancer immunotherapy. It did not erase fear, uncertainty, or the brutal realities of cancer. But it gave doctors and patients a new route through them.
Perhaps that is the most lasting experience of all: a shift from resignation to possibility. In cancers once known mainly for poor outcomes, immunotherapy created room for longer survival, deeper responses, and new therapeutic strategies. Not everyone benefits. Not every story ends well. But after Allison’s checkpoint breakthrough, more stories began with something that oncology never wastes: a real reason to believe the next chapter could be different.
Conclusion
The 2018 Nobel Prize in Medicine recognized more than an elegant scientific insight. It honored a turning point in cancer care. James P. Allison’s work on CTLA-4 showed that disabling an immune brake could help the body fight tumors, helping launch the era of immune checkpoint inhibitors. That breakthrough reshaped melanoma treatment, accelerated the rise of modern cancer immunotherapy, and created a blueprint for therapies that continue to expand across oncology.
The story is not tidy, and that is part of what makes it important. Checkpoint blockade offers real benefit, but not universal benefit. It creates new possibilities, but also new toxicities and new scientific puzzles. Still, the legacy of Allison’s work is unmistakable. He helped move cancer treatment from attacking the disease alone to empowering the immune system to join the fight. For a Nobel Prize, that is more than worthy. For patients, it is history with consequences.