
Table of Contents >> Show >> Hide
- What Is PCOS?
- What Is Endometrial Cancer?
- How PCOS and Endometrial Cancer Are Connected
- How Much Does PCOS Increase Endometrial Cancer Risk?
- Warning Signs You Shouldn’t Ignore
- How Doctors Evaluate the Uterine Lining
- Lowering Your Risk: What You Can Actually Do
- Talking with Your Healthcare Team
- Real-Life Experiences: Navigating PCOS and Cancer Concerns
- Conclusion
If you live with polycystic ovary syndrome (PCOS), you probably know the usual
suspects: irregular periods, stubborn weight, acne that didn’t get the memo
you’re an adult now, and hair growing in all the wrong places. What many
people don’t realize is that PCOS is also connected to something much more
seriousan increased risk of endometrial cancer. That sounds scary, but
understanding the link is actually one of the best tools you have to protect
yourself.
In this in-depth guide, we’ll break down how PCOS affects your uterus,
why hormones play such a big role, which symptoms deserve immediate
attention, and what you can dostarting nowto help manage your risk. We’ll
also share real-life experiences that show you’re not alone in navigating
PCOS and endometrial cancer concerns.
What Is PCOS?
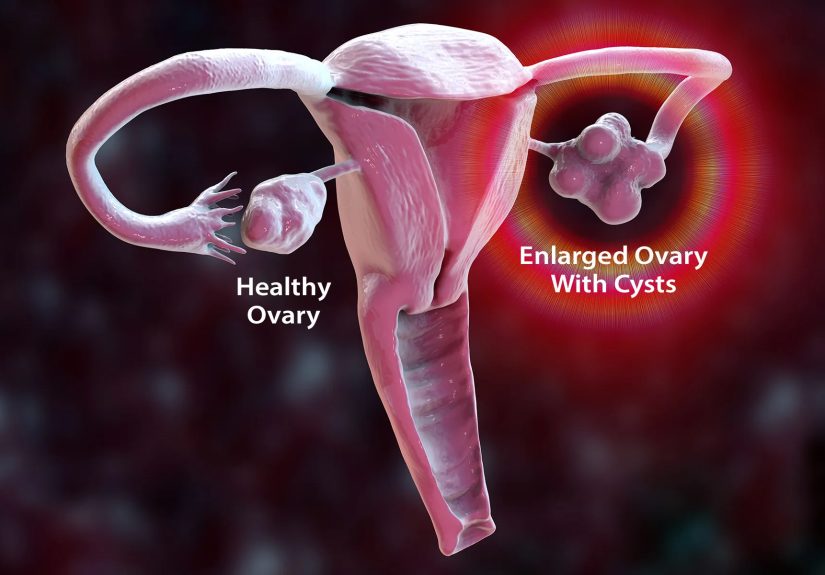
Polycystic ovary syndrome is a common hormone condition that affects people
with ovaries, often starting in the teen or young adult years. With PCOS,
the ovaries and other glands produce different levels of hormones than
usual, especially higher levels of androgens (often called “male hormones”),
along with insulin resistance in many people.
Common features of PCOS include:
- Irregular, infrequent, or very long menstrual cycles
- Signs of high androgens, like excess facial or body hair or acne
- Difficulty ovulating, which can lead to infertility
- Weight gain or difficulty losing weight, especially around the abdomen
- Insulin resistance and higher risk of type 2 diabetes or prediabetes
One of the biggest issues for the uterus is that people with PCOS often do
not ovulate regularly. That irregular ovulation is the bridge between PCOS
and endometrial problems, including cancer.
What Is Endometrial Cancer?
Endometrial cancer is a type of uterine cancer that starts in the lining of
the uterus, called the endometrium. This lining thickens every cycle under
the influence of hormones so that, if pregnancy occurs, it can support a
developing embryo. If pregnancy does not happen, the lining sheds as a
period.
In simple terms, endometrial cancer develops when cells in this lining begin
to grow in abnormal, uncontrolled ways. Over time, these abnormal cells can
become cancerous. Endometrial cancer is often diagnosed after menopause, but
it can occur earlier, especially when risk factors like obesity, chronic
anovulation (not ovulating), or hormonal imbalances are present.
One reason endometrial cancer is considered “hormone-related” is that
estrogen and progesterone strongly influence how the lining grows and sheds.
When estrogen’s growth-promoting effect is not balanced by progesterone, the
endometrium can become too thick and unstable, sometimes progressing from
overgrowth (hyperplasia) to cancer.
How PCOS and Endometrial Cancer Are Connected
1. Chronic Anovulation and “Unopposed” Estrogen
In a typical menstrual cycle, ovulation triggers the ovary to produce
progesterone. Progesterone acts like estrogen’s responsible friend: it
stabilizes the lining, matures it, and then helps it shed in a controlled
way during a period.
In PCOS, ovulation often doesn’t happen regularlyor sometimes not at all.
When you don’t ovulate, you don’t produce normal amounts of progesterone,
but your body may still be making estrogen (from the ovaries and from body
fat). This situation is called unopposed estrogen, meaning
estrogen is acting on the uterine lining without enough progesterone to keep
it in check.
Over time, this unopposed estrogen can cause:
- Endometrial thickening (endometrial hyperplasia)
- Irregular, heavy, or unpredictable bleeding
- Changes in cells that may progress to precancerous lesions
- In some cases, development of endometrial cancer
This is the core hormonal pathway linking PCOS and higher endometrial cancer
risk: fewer ovulations → less progesterone → prolonged unopposed estrogen →
overstimulation of the uterine lining.
2. Obesity, Insulin Resistance, and Metabolic Health
Many, though not all, people with PCOS have insulin resistance and are more
likely to have overweight or obesity. Excess body fatespecially around the
abdomenisn’t just “storage space.” It’s hormonally active. Fat tissue can
convert androgens into estrogen, adding even more estrogen to the system.
This combination of insulin resistance and higher estrogen levels from fat
tissue can:
- Further increase the amount of estrogen acting on the endometrium
- Raise the risk of endometrial hyperplasia and cancer
- Contribute to other risk factors like type 2 diabetes and high blood pressure
That’s why weight management and metabolic health are often front and center
in conversations about PCOS and long-term cancer riskthis isn’t just about
appearance; it’s about hormone chemistry and cellular health.
3. Other Overlapping Risk Factors
PCOS doesn’t exist in a vacuum. Many people with PCOS also live with other
conditions that can influence endometrial cancer risk, such as:
- Type 2 diabetes or prediabetes
- High blood pressure or high cholesterol
- Low levels of physical activity
- Family history of endometrial or colon cancer
Not everyone with PCOS will have these additional risk factors, and not
everyone with these risk factors has PCOS. But when they overlap, the risk
picture becomes strongerand that makes proactive monitoring even more
important.
How Much Does PCOS Increase Endometrial Cancer Risk?
Studies suggest that people with PCOS have a noticeably higher risk of
developing endometrial cancer compared with people without PCOS. Some
research has found that the risk can be about two to three times higher in
certain groups, especially when irregular periods, obesity, and long-term
unopposed estrogen are present.
That said, increased risk does **not** mean that endometrial cancer is
inevitable. Think of risk like the weather forecast: a higher chance of
rain doesn’t guarantee a downpour, but it does mean you’re wise to carry an
umbrella. In this case, your “umbrella” includes regular medical care,
paying attention to abnormal bleeding, and managing PCOS and metabolic
health over time.
Warning Signs You Shouldn’t Ignore
One advantageif we can call it thatof endometrial cancer is that early
warning signs often involve changes you can see: your bleeding pattern. For
anyone with PCOS, it can be tempting to dismiss irregular periods as “just
part of the condition.” However, certain changes deserve immediate medical
attention.
Talk with a healthcare professional as soon as possible if you notice:
- Bleeding or spotting between periods that’s new or worsening
- Very heavy periods (soaking pads or tampons every hour for several hours)
- Any bleeding after menopause
- Periods that suddenly become much longer or more painful than usual
- Persistent pelvic pain or pressure that doesn’t improve
These symptoms do not automatically mean cancerfar from it. They can be
caused by fibroids, hormonal shifts, or other benign conditions. But they
are red flags that the endometrium may not be behaving normally and
deserve professional evaluation.
How Doctors Evaluate the Uterine Lining
If your healthcare provider is concerned about your bleeding pattern or
overall risk, they may recommend tests to assess the endometrium. Common
options include:
- Pelvic ultrasound: Uses sound waves to estimate the
thickness of the uterine lining and look for fibroids or polyps. - Endometrial biopsy: A small sample of tissue from the
lining is collected and examined under a microscope to look for
hyperplasia (overgrowth) or cancer. - Hysteroscopy: A thin camera is passed through the cervix
to view the inside of the uterus and guide biopsies if needed.
An endometrial biopsy is often the key test to determine whether cells are
normal, precancerous, or cancerous. If changes are caught at an early or
precancerous stage, they can often be treated before cancer fully develops.
Lowering Your Risk: What You Can Actually Do
You can’t change the fact that you have PCOS, and you don’t control your
genes or the hormones you were born with. But there are practical steps
that may help reduce endometrial cancer risk and support overall health.
1. Manage Menstrual Regularity
One major goal in PCOS care is to avoid long stretches of time without a
period, because that usually means the lining has been exposed to
unopposed estrogen. Your healthcare provider may recommend treatments such
as:
- Combined hormonal contraceptives (pill, patch, ring)
to provide both estrogen and progestin on a regular schedule - Progestin-only options, such as a hormone-releasing
IUD or periodic progestin pills, to thin and stabilize the lining - Other individualized hormone approaches depending on your goals,
including whether you want to become pregnant
The exact approach depends on your age, health history, and pregnancy
plans, so this is a conversation to have directly with your provider rather
than a one-size-fits-all solution.
2. Support a Healthy Weight and Metabolism
Weight can be a sensitive topic, especially when you feel like you’ve
“tried everything.” PCOS makes weight management more challenging, but even
modest weight loss in people with overweight or obesity can help:
- Reduce insulin resistance
- Lower estrogen production from body fat
- Improve ovulation patterns for some people
- Decrease overall risk of endometrial cancer and other conditions
Approaches that combine nutrition, physical activity, stress management,
and sometimes medication (such as insulin-sensitizing drugs) can be more
effective than focusing on diet alone. Think sustainable changes, not crash
diets. Your future selfand your uteruswill thank you.
3. Stay on Top of Other Health Conditions
Because PCOS is often linked with other metabolic issues, it’s important to
stay current on screening for:
- Prediabetes and diabetes
- High blood pressure
- High cholesterol or triglycerides
- Sleep apnea, especially if you have loud snoring or daytime fatigue
Managing these conditions doesn’t just protect your heart and blood vessels;
it may indirectly lower cancer risk by improving hormonal and metabolic
balance.
Talking with Your Healthcare Team
If you have PCOS, it’s reasonableand healthyto ask your doctor directly
about your endometrial cancer risk. Good questions might include:
- “Given my PCOS and weight, how high is my risk of endometrial cancer?”
- “How long is too long to go without a period before we should check my uterine lining?”
- “Would I benefit from regular progestin therapy or a hormonal IUD?”
- “Are there any warning signs that should send me to the clinic right away?”
A supportive healthcare provider will not dismiss your concerns or blame
you for your symptoms. Instead, they will work with you to create a plan
that fits your body, your lifestyle, and your goals.
Real-Life Experiences: Navigating PCOS and Cancer Concerns
Statistics and hormone diagrams are helpful, but they don’t always capture
what it feels like to live in a body with PCOS while hearing about cancer
risks. The following experiences are composite stories based on common
patterns people report. They’re not about one specific person, but they may
sound familiar.
“I Thought Skipping Periods Was Just Convenient”
In her early twenties, Alex had what many of her friends enviedonly a
couple of periods a year. She had been told she had PCOS during college,
but life was busy, she felt mostly fine, and not having periods seemed like
a win. She didn’t want to get pregnant yet, so she never pushed for
follow-up.
In her early thirties, she started having random episodes of very heavy
bleeding, soaking through pads and clothes at work. At first, she brushed
it off as “PCOS acting up,” but eventually the exhaustion and anxiety sent
her to a gynecologist. An ultrasound showed a thickened endometrial lining,
and a biopsy revealed precancerous changes (atypical hyperplasia).
The good news: because the changes were caught before invasive cancer
developed, she had more options. Her doctor recommended high-dose progestin
therapy and close follow-up. Over the next year, her biopsies gradually
normalized. The experience shook herbut it also changed how she viewed her
PCOS. Skipping periods was no longer “convenient”; it was a signal her
uterus needed attention.
“I Did Everything ‘Right’ and Still Felt Worried”
Taylor was diagnosed with PCOS at 16. She started hormonal birth control
soon after to regulate her cycles and help with acne. She exercised,
maintained a relatively stable weight, and saw her clinician regularly.
Even so, every time she read an article about PCOS and cancer risk, her
stomach dropped.
Her provider took her concerns seriously. They walked through her personal
risk factors, family history, and current treatment. Together, they decided
on periodic check-ins and clear guidelines: if she ever experienced
bleeding between periods or after stopping hormone therapy, she would come
in promptly.
Taylor still had moments of anxietyDr. Google is persistentbut having a
plan and a provider who answered her questions without minimizing them made
a huge difference. She learned that “increased risk” does not mean “it’s
just a matter of time,” especially when you’re proactive.
“Weight, PCOS, and Shame: Breaking the Cycle”
For Jordan, the hardest part of PCOS wasn’t the irregular periodsit was
the constant pressure about weight. Every appointment seemed to start and
end with the scale. She knew her weight was a risk factor for diabetes and
endometrial cancer, but the way it was discussed left her feeling defeated
instead of motivated.
Eventually, she switched to a provider who approached the topic
differently. Together, they focused on small, realistic changes: walking
most days, improving sleep, and working with a dietitian who understood
PCOS. Instead of chasing a “perfect” weight, they focused on health markers
like blood sugar levels, blood pressure, and how she felt day to day.
Over time, Jordan lost a modest amount of weight, but more importantly, her
cycles became more regular and her energy improved. Her risk of endometrial
cancer didn’t disappear, but she felt more in control and less ashamed. She
realized that PCOS management and cancer prevention are long games, not
crash projects.
You’re Not Alone in This
If you’ve ever googled “PCOS and endometrial cancer” at 2 a.m. and felt
your heart pounding, you’re far from alone. Many people only learn about
this link in passing or after a scare. The important thing to remember is
that risk is not destiny.
You can:
- Pay attention to your bleeding patterns and speak up about changes
- Ask your healthcare provider directly about your uterus and cancer risk
- Use hormonal treatments when appropriate to protect your endometrium
- Work on sustainable habits that support your metabolic health
- Seek compassionate, informed carebecause you deserve it
PCOS may change your hormone landscape, but with knowledge, monitoring, and
support, you can reduce risks and make informed choices about your health
at every stage of life.
Conclusion
PCOS and endometrial cancer are closely linked through hormones, especially
the long-term effects of unopposed estrogen and chronic anovulation.
Metabolic factors like obesity and insulin resistance add to the picture,
but they are also areas where lifestyle, medical treatment, and regular
follow-up can make a real difference.
Understanding the connection doesn’t mean living in fearit means knowing
what to watch for, when to seek evaluation, and how to partner with your
healthcare team. With the right information and support, PCOS can be
managed in a way that not only improves daily symptoms but also protects
your long-term uterine health.





