Table of Contents >> Show >> Hide
- What Exactly Is Rheumatoid Arthritis?
- Symptoms: What RA Can Feel Like (and Where It Shows Up)
- Causes and Risk Factors: Why Does RA Happen?
- Diagnosis: How Doctors Confirm RA
- Treatment: How RA Is Managed (and Why Early Matters)
- Prevention: Can You Prevent Rheumatoid Arthritis?
- When to See a Doctor (and What to Ask)
- Living With RA: Day-to-Day Strategies That Add Up
- Experiences Related to RA: What People Commonly Describe (Added Section)
- Conclusion
Rheumatoid arthritis (RA) is what happens when your immune systemthe body’s usually-helpful security teamgets a little too enthusiastic and starts frisking the wrong people. Instead of targeting germs, it targets your own joints (and sometimes other organs), causing inflammation, pain, stiffness, and gradual damage if it isn’t brought under control.
If you’ve ever woken up with hands that feel like they spent the night turning into creaky, stubborn mittens, you’re not alone. RA is common, treatable, andthis is the important partvery much a “the sooner, the better” condition. Early diagnosis and early treatment can make a huge difference in preventing long-term joint damage and keeping you doing the things you like (including opening jars without negotiating with them).
What Exactly Is Rheumatoid Arthritis?
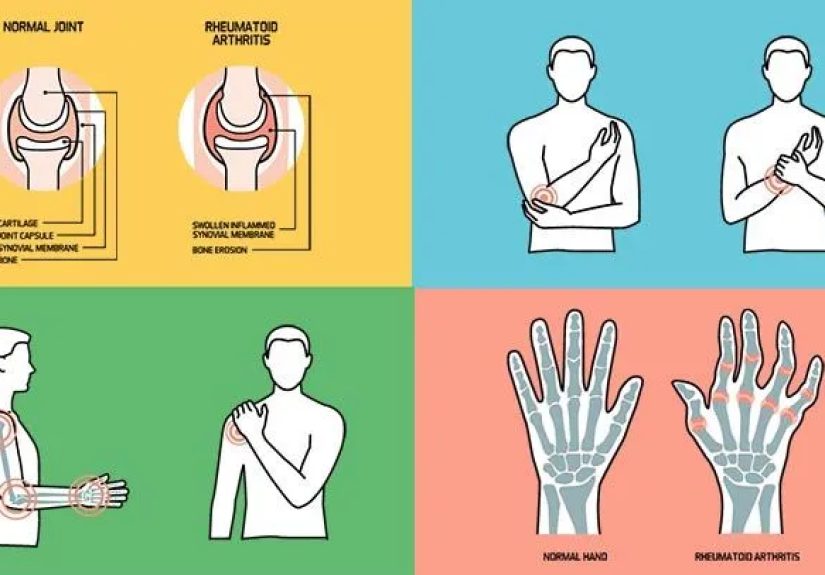
RA is a chronic autoimmune disease. “Chronic” means it can last a long time. “Autoimmune” means the immune system mistakenly attacks the body’s own tissues. In RA, the main target is the lining of your joints (the synovium). When that lining stays inflamed, it can thicken, joints can swell, and over time the cartilage and bone around the joint can be damaged.
RA vs. Osteoarthritis: Not the Same Movie
RA is often confused with osteoarthritis (OA), but they’re different conditions with different causes. OA is more about “wear and tear” over timecartilage breaking down from aging, overuse, or injury. RA is more like an internal miscommunication: the immune system drives inflammation that can affect joints and also body systems beyond the joints.
Symptoms: What RA Can Feel Like (and Where It Shows Up)
RA symptoms can start gradually or come on more noticeably. Some people have mild symptoms at first; others get hit with a bigger wave. Either way, RA tends to have patterns that help clinicians recognize it.
Common joint symptoms
- Pain, swelling, warmth, and tenderness in one or more joints
- Stiffness that’s usually worse in the morning or after resting (often lasting 30–60+ minutes)
- Symmetry: symptoms commonly affect the same joints on both sides of the body (both wrists, both hands, both feet)
- Small joints are frequent early targetshands, wrists, and feetthough larger joints can be involved too
Whole-body symptoms (yes, RA can be extra)
RA isn’t just “joint stuff.” Many people also notice:
- Fatigue (the kind that laughs at your coffee)
- Low-grade fever once in a while
- Reduced appetite or generally feeling “off”
Flares and remission
RA often cycles. Symptoms may worsen during flares and ease during periods of low activity or remission. Triggers aren’t always obvious, but stress, smoking exposure, infections, overdoing it physically, or stopping medications suddenly can sometimes be involved.
Symptoms beyond the joints
Because RA is a systemic inflammatory disease, it can affect other areas. Depending on the person and disease severity, this can include: dry eyes/mouth, anemia, rheumatoid nodules (firm bumps under the skin), and inflammation involving blood vessels, the lungs, or tissues around the heart. Not everyone gets these, but they matter because they influence treatment choices and monitoring.
Causes and Risk Factors: Why Does RA Happen?
The short answer: we don’t have a single “Aha!” cause. The longer, more accurate answer: RA likely develops from a mix of genetic susceptibility and environmental exposures that affect immune behavior over time.
What researchers believe is going on
In RA, the immune system becomes dysregulatedmeaning it starts reacting as if joint tissues are the enemy. This leads to ongoing inflammation in the joint lining, which can drive swelling, pain, and eventually structural damage.
Risk factors that can increase the odds
- Age: RA can happen at any age, but risk increases with age.
- Sex: RA is more common in women than men (hormonal factors may play a role).
- Family history/genetics: having a relative with RA modestly increases risk.
- Smoking: long-term smoking increases risk and is linked with more severe disease.
- Obesity: may increase risk and can make disease harder to improve.
- Periodontitis (gum disease): associated with developing RA in some research.
- Certain lung diseases: also associated with RA development in some studies.
Diagnosis: How Doctors Confirm RA
RA diagnosis is a bit like detective work: no single test is “the RA test,” so clinicians combine your symptoms, exam findings, labs, and imaging. A primary care clinician may start the process, but many people are diagnosed and managed by a rheumatologist (a specialist in inflammatory and autoimmune joint diseases).
1) Medical history and symptom pattern
Expect questions like: When did symptoms start? Which joints? Is there morning stiffness? How long does it last? Are daily tasks harder? Clinicians also ask about family history and other medical conditions.
2) Physical exam
The exam focuses on joint swelling, tenderness, range of motion, function (how you walk, bend, grip), and signs such as nodules or rashes. Because RA can affect the lungs and heart, clinicians may also listen to your chest for signs of inflammation.
3) Lab tests
Common blood tests include:
- Rheumatoid factor (RF): can support the diagnosis, but it’s not exclusive to RA.
- Anti-CCP antibodies: often seen in RA and may appear before symptoms, helping with early diagnosis.
- ESR and CRP: markers of inflammation used to assess activity and monitor response to treatment.
- Complete blood count (CBC): can help identify anemia, which is common in RA.
Important nuance: some people have RA with normal RF and anti-CCP. So “negative bloodwork” doesn’t always mean “no RA.”
4) Imaging
X-rays can help monitor changes over time, but early RA may not show obvious changes on X-ray. Ultrasound and MRI can detect inflammation and early joint damage sooner in some cases.
Treatment: How RA Is Managed (and Why Early Matters)
There’s no cure yet, but RA is highly treatableand outcomes are far better now than they were decades ago. Modern RA care aims to: reduce inflammation, relieve pain, protect joints and organs, and keep you functional and active.
The big idea: treat early, treat to a target
Joint damage can begin early in the disease course, and once damage happens it often can’t be fully reversed. That’s why clinicians push for early diagnosis and early use of medications that change the disease trajectorynot just those that mask symptoms.
Many treatment plans use a treat-to-target approach: you and your clinician choose a goal (remission or low disease activity) and adjust therapy until you get therethen maintain and monitor.
Medications used in RA
1) DMARDs: the foundation
DMARD stands for disease-modifying antirheumatic drug. These medications calm the immune-driven inflammation and help prevent joint damage. For many people, a conventional DMARDoften methotrexateis a first-line option.
- Methotrexate (common first choice)
- Hydroxychloroquine (often for milder disease or in combination)
- Sulfasalazine
- Leflunomide
Methotrexate is frequently recommended as initial therapy for people with moderate-to-high disease activity, and many guidelines prioritize methotrexate monotherapy before stepping up to more advanced options if needed.
2) Biologic DMARDs
If conventional DMARDs aren’t enough, clinicians may add or switch to biologic therapiestargeted drugs that block specific immune pathways involved in inflammation.
Examples include TNF inhibitors (like adalimumab or etanercept) and other biologics (such as abatacept or tocilizumab). Biologics can be very effective, but because they affect immune function, they can raise infection riskso monitoring and vaccination planning are part of smart care.
3) Targeted synthetic DMARDs (JAK inhibitors)
JAK inhibitors (such as tofacitinib, baricitinib, and upadacitinib) are oral targeted therapies used for some people whose disease isn’t well controlled with other options. They can be highly effectivebut they also come with important safety considerations.
The FDA has required boxed warnings for certain JAK inhibitors about increased risks of serious heart-related events, cancer, blood clots, and death in some patient populations. This doesn’t mean “never use them”it means the decision should be individualized, weighing benefits and risks with your clinician, especially if you have cardiovascular risk factors or a history of cancer.
4) NSAIDs and pain relief options
Nonsteroidal anti-inflammatory drugs (NSAIDs) can help with pain and swelling, but they don’t prevent joint damage on their own. Think of NSAIDs as comfort measures while the DMARDs do the heavy lifting.
5) Corticosteroids (steroids): useful, but not a long-term bestie
Steroids (like prednisone) can quickly reduce inflammation and are sometimes used short-term as a “bridge” while DMARDs ramp up. However, many guidelines emphasize minimizing steroid use due to potential harmsespecially with longer-term useso clinicians often prefer adjusting DMARDs rather than keeping steroids around indefinitely.
Non-medication treatments that matter
- Physical and occupational therapy: improve function, protect joints, and teach energy-saving strategies.
- Exercise: tailored movement supports strength, flexibility, and fatigue management.
- Assistive tools: splints, ergonomic grips, and adaptive devices reduce strain.
- Surgery: sometimes considered when joints are severely damaged (for example, joint replacement).
Monitoring and safety
Because RA and RA medications can affect the immune system and other organs, follow-up isn’t optionalit’s part of the treatment. Monitoring may include labs, periodic imaging, and screening for complications like osteoporosis (especially if steroids are involved). Clinicians may recommend certain vaccines to help lower the risk and severity of infections.
Prevention: Can You Prevent Rheumatoid Arthritis?
There’s no guaranteed way to prevent RAbecause we can’t fully control genetics or predict immune misfires. But you can reduce risk and improve outcomes by focusing on modifiable factors and early action.
Risk-reduction steps that are actually practical
- Don’t smoke (and quit if you do): smoking is one of the strongest modifiable risk factors and is linked with worse RA.
- Work toward a healthy weight: obesity may increase risk and can make disease harder to improve.
- Take gum health seriously: periodontitis is associated with RA in some researchregular dental care is a smart move.
- Don’t ignore persistent joint symptoms: early evaluation can prevent damage, even if the final diagnosis isn’t RA.
When to See a Doctor (and What to Ask)
Consider making an appointment if you have joint swelling, pain, and morning stiffness that lasts weeks, especially if it’s on both sides of your body or involves the hands, wrists, or feet. A simple “wait and see” approach can cost time your joints would rather keep.
Questions that can help you advocate for yourself
- Could this be inflammatory arthritis (not just wear-and-tear arthritis)?
- Which tests do you recommend (RF, anti-CCP, ESR/CRP, imaging)?
- Should I see a rheumatologist?
- What’s the treatment goalremission or low disease activityand how will we measure it?
- What side effects should I watch for, and what monitoring will I need?
Living With RA: Day-to-Day Strategies That Add Up
Good RA care is a combination of the right medication plan and the right lifestyle supports. Many people find that small daily choices make a big difference: pacing activity, protecting joints, prioritizing sleep, building strength gently, and communicating openly with their care team.
If fatigue is one of your main symptoms, treat it like a real symptom (because it is). Planning rest breaks, using labor-saving tools, and adjusting routines can be as important as any single workout plan. Also: support counts. Whether that’s family, friends, counseling, or a support group, RA is easier when you’re not white-knuckling it alone.
Experiences Related to RA: What People Commonly Describe (Added Section)
When people talk about rheumatoid arthritis, the first thing they often mention isn’t even painit’s the strange unpredictability. One day you can type, cook, and carry groceries like usual. The next day, your fingers feel stiff and swollen, and buttoning a shirt becomes an Olympic event. Many people describe morning stiffness as the giveaway: it’s not just “a little creaky,” it’s a prolonged “warm-up period” where joints don’t feel cooperative until they’ve been moving for a while.
Another common theme is how long it can take to feel believed. Because symptoms can come and go, people may worry they’re overreactingespecially if early blood tests are negative. Some describe a frustrating cycle: pain and stiffness flare up, then ease right before the appointment, making it harder to explain what’s happening. Keeping a symptom diary (which joints, how long morning stiffness lasts, what activities became harder) is something many patients wish they had started earlier. It gives the clinician clearer clues and helps you spot patterns.
After diagnosis, emotions tend to come in a mixed bag: relief at having an answer, worry about the future, and confusion over medication names that sound like they were invented in a science fiction writers’ room. Many people say the biggest mindset shift is learning that RA treatment is not only about feeling better todayit’s about preventing damage next year. That’s why DMARDs matter even when pain relievers seem to “work.” People often notice that once the right DMARD regimen kicks in, everyday life slowly returns: grip strength improves, fatigue eases, and flares become less frequent or less intense.
Medications can involve trial and error. Some people do well on the first DMARD; others need dose adjustments, combination therapy, or a step up to biologics or targeted therapies. A frequent real-world experience is learning the “monitoring routine”: periodic lab checks, infection awareness, and vaccine planning. Many patients also describe becoming better at pacingdoing tasks in smaller chunks, using adaptive tools, and prioritizing joint-friendly movement rather than all-or-nothing workouts.
Social and work life can be part of the journey too. People often share that it helps to explain RA in practical terms to others: “My joints might look fine, but inflammation makes them act up,” or “I’m not lazyI’m managing fatigue.” When friends, family, teachers, or coworkers understand that symptoms can fluctuate, it reduces stress (and stress itself can be a flare fuel). Over time, many people learn that asking for help isn’t defeat; it’s strategy. The goal isn’t to “push through” foreverit’s to keep doing what you love in a sustainable way.
Note: These are common experiences people report, not medical advice. If you suspect RA or have persistent joint symptoms, a clinician can help you get the right evaluation and plan.
Conclusion
Rheumatoid arthritis is a chronic autoimmune condition that can affect jointsand sometimes much morebut it’s also one of the success stories of modern medicine when caught and treated early. If you notice persistent joint swelling, symmetrical pain, and morning stiffness that doesn’t quit, it’s worth getting evaluated. With early diagnosis, DMARD-based treatment, smart monitoring, and supportive daily strategies, many people reach remission or low disease activity and keep living full, active liveswithout having to negotiate with every doorknob.