


Sarcasm memes have become the internet’s favorite way to laugh at stress, awkward moments, work chaos, social...
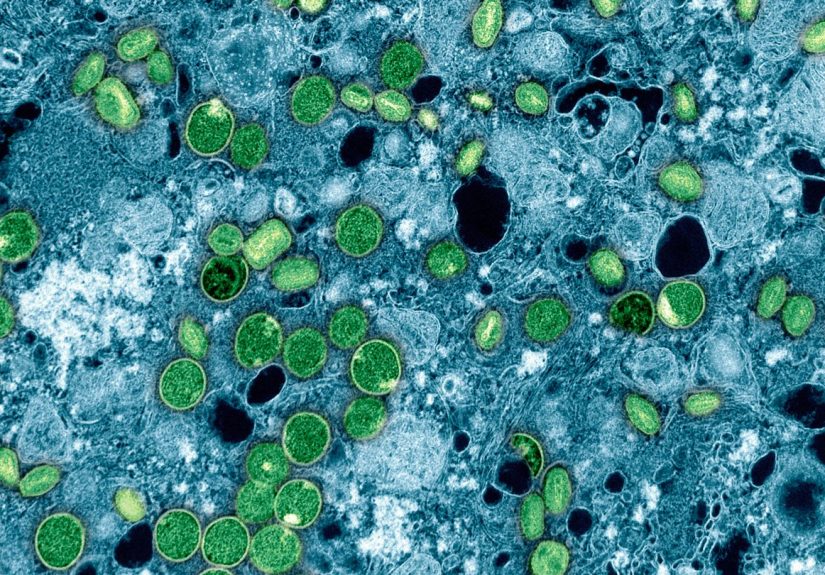
Clade I mpox is no longer only a distant concern: more than 20 cases had been reported...
Some Twitter pages start off quirky and quickly escalate into a full-blown surreal comedy universe. This in-depth,...
Hair looking thinner since perimenopause or menopause began? You’re far from alone. Up to half of women...
Zote laundry soap has a cult following for a reason. This giant old-school soap bar is a...

Exposure therapy is one of the most effective psychological treatments for fear and anxiety-based conditions like phobias,...

If getting dressed feels like autopilot, you might be in a style rutand it’s more common than...

Drew Barrymore did not want a standard talk-show set with a couch, a desk, and enough shine...
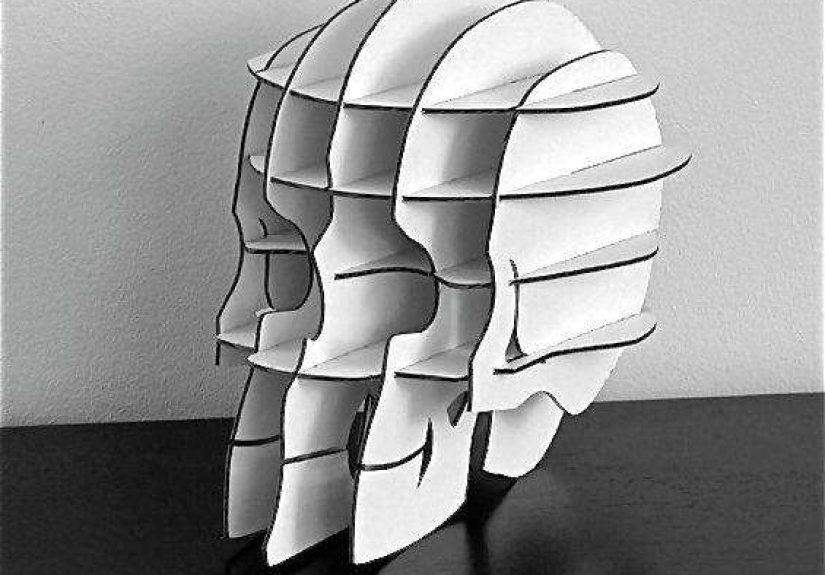
The Cardboard Safari flat-pack skull (often called Vince) is more than quirky décorit’s a clever blend of...

Achy joints? You’re not alone. This guide breaks down the 10 best joint supplements of 2025, selected...