Table of Contents >> Show >> Hide
- What Is a Radio Controlled Pacemaker?
- Why Wireless Pacemakers Became a Cybersecurity Concern
- The 2017 Abbott/St. Jude Pacemaker Firmware Update
- Does “Easily Hacked” Mean Anyone Can Do It?
- How Remote Monitoring Helps Patients
- What Regulators Expect From Medical Device Makers
- Where the Real Risk Often Lives
- What Patients Should Actually Do
- What Hospitals and Clinics Should Do
- Why Responsible Disclosure Matters
- Experience-Based Reflections: What This Topic Teaches Us
- Conclusion
It sounds like the plot of a medical thriller: a tiny device inside someone’s chest, a mysterious radio signal, and a hacker in a hoodie trying to play villain with a heartbeat. The reality is less cinematic, but still important. Modern pacemakers and other cardiac implantable electronic devices can communicate wirelessly with clinic programmers, home monitors, and remote monitoring systems. That wireless convenience helps doctors check device function, review heart rhythm data, and catch problems earlier. It also creates a cybersecurity question that medicine can no longer ignore: when a life-sustaining device talks by radio, who is allowed to talk back?
The title “Radio Controlled Pacemakers Are Easily Hacked” is deliberately bold, but the truth deserves nuance. Most pacemaker patients should not panic. There is no public evidence that ordinary patients are being routinely targeted through their implanted devices. At the same time, public safety communications and past device updates have shown that some radio-frequency-enabled cardiac devices have had real vulnerabilities. In other words, the danger is not science fiction, but it is also not as simple as someone waving a smartphone at a stranger in a grocery store and taking control of a heartbeat. The real story lives between those extremes.
What Is a Radio Controlled Pacemaker?
A pacemaker is a small battery-powered medical device that helps the heart maintain a safe rhythm when the natural electrical system is too slow or irregular. Traditional pacemakers usually include a pulse generator and one or more leads that deliver electrical impulses to the heart. Some newer devices are leadless or wireless in design, but the core purpose is the same: monitor rhythm, sense when help is needed, and deliver pacing when appropriate.
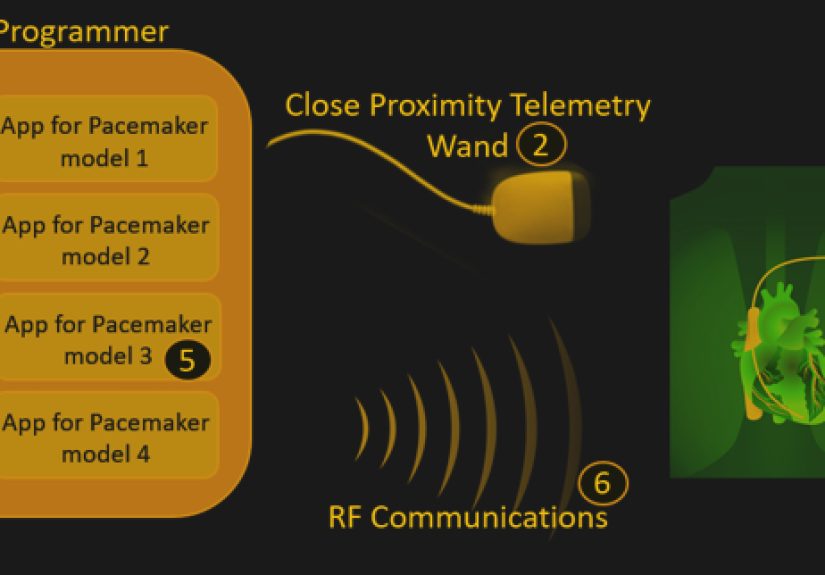
The phrase “radio controlled” does not mean a pacemaker is controlled like a toy car. It means the device may use radio frequency communication for certain approved medical functions. A clinic programmer may communicate with the implanted device during follow-up visits. A home monitor may collect device information and send it to a care team. In some systems, remote monitoring can reduce unnecessary office visits, speed up clinical response, and give doctors more timely information about battery status, abnormal rhythms, or device performance.
That is the good side of wireless medicine. The awkward side is that every communication channel needs security. If a medical device can receive instructions, those instructions must be authenticated. If it sends patient data, that data should be protected. If it relies on a home transmitter or clinic programmer, those companion systems also become part of the security story. A pacemaker is not just a metal-and-battery device anymore; it is part of a small health technology ecosystem.
Why Wireless Pacemakers Became a Cybersecurity Concern
Medical devices used to be mostly isolated. They were implanted, adjusted in a clinic, and checked during scheduled appointments. As remote monitoring became more common, devices gained the ability to communicate across short-range radio links and, through external equipment, into broader health care networks. That improved care, but it also expanded the attack surface.
The U.S. Food and Drug Administration has repeatedly noted that connected medical devices bring both benefits and cybersecurity risks. Wireless functions can help health care professionals remotely monitor patients, transfer data, and in some cases program devices. However, connected systems can be vulnerable to unauthorized access, data exposure, interference, or malfunction if security is weak. In health care, cybersecurity is not just an IT department problem. It is a patient safety issue wearing a name badge.
Cardiac devices are especially sensitive because their job is physical. A compromised laptop might leak files. A compromised medical device could affect therapy, alarms, battery use, or clinical decision-making. That does not mean every theoretical flaw becomes a real-world crisis. It means manufacturers, regulators, hospitals, and clinicians must treat software quality and radio security with the same seriousness as sterile technique and battery reliability.
The 2017 Abbott/St. Jude Pacemaker Firmware Update
The best-known example came in 2017, when Abbott, formerly St. Jude Medical, released a firmware update for certain radio-frequency-enabled implantable pacemakers and cardiac resynchronization therapy pacemakers. The update was intended to reduce the risk that an unauthorized user could access affected devices. The affected families included models such as Accent, Anthem, Assurity, and Allure. The update required an in-person visit with a health care provider and was not performed from home.
Public reporting at the time stated that about 465,000 implanted devices in the United States were affected. The concern was that, if exploited, the vulnerabilities could allow unauthorized access using commercially available equipment. Possible consequences included changes to device settings, rapid battery depletion, or inappropriate pacing. That sounds terrifying, and frankly, it should get attention. But context matters: regulators and health care organizations also reported no known patient harm tied to those vulnerabilities at the time of the communication.
Another important detail: the FDA and Abbott did not recommend removing and replacing affected pacemakers as a preventive measure. Why? Because surgery carries real risks. Cutting into a patient to replace a working implanted device can be more dangerous than applying a carefully planned firmware update. This is the heart of medical cybersecurity risk management: the safest answer is not always the most dramatic one.
Does “Easily Hacked” Mean Anyone Can Do It?
No. “Easily hacked” is a catchy phrase, but it can be misleading. In real life, exploiting a pacemaker vulnerability generally requires a combination of technical knowledge, proximity, compatible equipment, device-specific understanding, and opportunity. It is not like guessing a weak Wi-Fi password from across town. Many vulnerabilities described in public advisories are limited by physical range, specialized communication methods, clinical workflows, and manufacturer-specific systems.
That said, the fact that an attack is difficult does not make it irrelevant. Airplanes are difficult to hijack, but aviation security still matters. Bank vaults are difficult to crack, but banks do not leave the door open because most people are honest. Medical device security works the same way. The point is not that every attacker will succeed; the point is that life-critical technology should be designed so that failure is unlikely, detectable, and manageable.
The better question is not, “Can a pacemaker be hacked?” The better question is, “Has the system been designed to resist unauthorized access, receive timely updates, protect patient data, and keep delivering therapy safely even when something goes wrong?” That question is more boring than a movie plot, but it is much more useful.
How Remote Monitoring Helps Patients
It would be a mistake to talk about wireless pacemakers only as a danger. Remote monitoring is one of the major advances in cardiac device care. It can help clinics detect abnormal rhythms, battery issues, lead problems, and device alerts sooner than traditional scheduled visits alone. For patients who live far from a hospital, have mobility challenges, or need frequent checks, remote monitoring can make care more convenient and more responsive.
Think of it like a smoke alarm. A smoke alarm introduces electronics into your home, and electronics can fail. But nobody argues that the safest house is one with no alarm at all. The safest house has a well-designed alarm, fresh batteries, and someone who knows what to do when it beeps at 2 a.m. A connected pacemaker system works similarly. The goal is not to disconnect patients from care. The goal is to make connected care secure enough to trust.
Patients should never turn off or avoid remote monitoring because of scary headlines without talking to their clinician. In many cases, the clinical benefit of monitoring is far greater than the cybersecurity risk. A patient’s cardiologist or electrophysiology clinic can explain whether a specific device model has updates, alerts, or special instructions.
What Regulators Expect From Medical Device Makers
Medical device cybersecurity has matured significantly over the past decade. Current FDA expectations emphasize a total product life cycle approach. That means cybersecurity should be considered before a device reaches the market, while it is being used by patients, and when vulnerabilities are discovered after release.
Manufacturers of connected medical devices are expected to plan for vulnerability monitoring, coordinated vulnerability disclosure, updates, patches, and software transparency. A software bill of materials, often called an SBOM, helps identify commercial, open-source, and off-the-shelf components inside a device. That matters because a vulnerability in a common software library can affect many products at once. Without a component inventory, finding affected devices can become a scavenger hunt nobody wanted to play.
Modern guidance also encourages secure-by-design and secure-by-default thinking. In plain English, this means security should not be taped onto the product at the end like a last-minute Halloween costume. It should be built into the architecture from the start. Authentication, encryption, logging, update mechanisms, resilience, and incident response should be part of the design conversation early, not after a researcher finds a flaw.
Where the Real Risk Often Lives
When people imagine pacemaker hacking, they often picture the implanted device as the main target. In practice, the broader ecosystem may be just as important. Home monitors, clinic programmers, hospital networks, cloud services, vendor portals, and staff workflows all matter. A secure implant connected to a poorly managed external system is like a castle with a strong front gate and a back door labeled “please jiggle handle.”
Hospitals and clinics need strong asset management, network segmentation, software update processes, vendor coordination, and staff training. Manufacturers need clear security bulletins and update pathways. Researchers need safe ways to report vulnerabilities. Patients need understandable communication that explains what is known, what is not known, and what action is recommended. When any of these pieces fail, confusion fills the gap.
Medical cybersecurity is also complicated by device longevity. A pacemaker can remain implanted for years. Technology changes faster than the human body’s need for a stable heartbeat. A device designed under yesterday’s threat model may still be in a patient’s chest when tomorrow’s attacks are being discussed. That is why postmarket monitoring and patch planning matter so much.
What Patients Should Actually Do
For patients with a pacemaker or other cardiac implantable electronic device, the most useful response is calm, practical, and boringin the best possible way. Keep scheduled follow-up appointments. Use the home monitor as instructed. Ask the device clinic whether the device model has any safety notices, firmware updates, or manufacturer recommendations. Report unusual symptoms promptly. Keep contact information current with the clinic and device manufacturer if enrollment is required for safety updates.
Patients should not attempt to modify, shield, disconnect, or “secure” the device themselves. Homemade cybersecurity experiments and implanted medical devices are a terrible pairing, like fireworks and a gas station. Device settings should be changed only by qualified medical professionals using approved equipment. If a patient receives a letter about an update, the right move is to call the care team, not to panic-search forums at midnight.
It is also reasonable to ask direct questions before implantation or during follow-up: Does this device use remote monitoring? How are updates handled? Who contacts me if a vulnerability is found? What should I do if my monitor stops working? Are there any cybersecurity notices for my device model? Good clinicians may not have every technical detail memorized, but they should be able to connect patients with reliable answers.
What Hospitals and Clinics Should Do
Health care organizations have a bigger job. They should maintain an accurate inventory of connected medical devices, including model numbers, software versions, network connections, and support status. They should segment networks so that medical devices are not casually sharing digital hallways with every laptop, printer, and vending machine that accepts mobile payments. They should review vendor advisories, test update processes, and create response plans for cybersecurity events that could affect patient care.
Clinics should also prepare communication templates before a crisis. Patients do not need a PhD in cryptography to understand risk, but they do need plain language. A good notice explains who is affected, what the issue could do, whether any harm has been reported, what action is recommended, and why the recommended action is safer than alternatives. “Please don’t panic, but also please show up” is a delicate message. It should not be improvised at 4:55 p.m. on a Friday.
Why Responsible Disclosure Matters
Security researchers have played an important role in identifying weaknesses in medical devices. Responsible disclosure allows researchers, manufacturers, regulators, and clinicians to coordinate fixes before information creates unnecessary risk. The goal is not to embarrass companies or frighten patients. The goal is to close gaps in technology that people depend on to stay alive.
However, public communication must be handled carefully. Too little disclosure leaves patients uninformed. Too much technical detail can create a road map for misuse. The best communication gives enough information to support trust and action without turning a safety notice into a tutorial. In medical device cybersecurity, restraint is not secrecy; it is part of harm reduction.
Experience-Based Reflections: What This Topic Teaches Us
Anyone who has followed medical technology over the last decade can see a pattern: health care innovation often moves faster than public understanding. A patient receives a pacemaker and thinks of it as a medical device, while engineers see software, wireless protocols, firmware, update channels, authentication, cloud systems, and data flows. Both views are correct. The device is a medical lifeline and a small computer. The problem begins when only one of those truths gets attention.
One practical experience from this topic is that fear spreads faster than facts. When headlines say pacemakers can be hacked, many readers imagine immediate danger. But when clinicians explain that known advisories usually involve specific models, specific conditions, and managed updates, the conversation becomes more balanced. Patients deserve that balance. They should not be dismissed with “don’t worry about it,” and they should not be frightened into thinking their chest contains a remote-controlled disaster.
Another lesson is that software maintenance is now part of medical care. In the old days, people expected updates for computers and phones, not implants. Today, a firmware update can be a safety measure. That shift feels strange because medical devices have historically been associated with permanence and reliability. But reliability now includes the ability to respond to newly discovered risks. A device that can be updated safely may be more secure over time than a device frozen forever in its original state.
There is also an experience lesson for hospitals: cybersecurity cannot be delegated entirely to the IT department. Device nurses, electrophysiologists, biomedical engineers, procurement teams, compliance officers, and vendors all touch the process. If a clinic does not know which patients have which models, a security advisory becomes a detective story. If procurement buys connected devices without asking about updates and support, the organization inherits risk wrapped in shiny packaging. If staff are not trained, even good security features may be underused.
For manufacturers, the lesson is equally clear: trust is part of the product. Patients cannot inspect the code inside a pacemaker. They cannot personally verify encryption, authentication, or update integrity. They trust regulators, clinicians, and manufacturers to make those decisions responsibly. When a vulnerability appears, the quality of the response matters almost as much as the flaw itself. Clear communication, timely patches, and honest risk assessment can preserve confidence. Silence, delay, and vague language do the opposite.
For writers and publishers, the topic is a reminder that dramatic titles need responsible content. “Radio Controlled Pacemakers Are Easily Hacked” may attract clicks, but an article should not leave readers with a cartoon version of reality. The better story is deeper: connected cardiac devices improve care, wireless communication introduces risk, past vulnerabilities prove the risk is real, and modern regulation is pushing the industry toward stronger security. That is less sensational than a hacker movie, but far more useful.
Finally, this topic teaches that safety is not the absence of technology. Safety is good technology, maintained well, explained clearly, and monitored continuously. A pacemaker that communicates wirelessly is not automatically unsafe. A disconnected device is not automatically safer. The safest path is thoughtful design, careful clinical use, fast vulnerability response, and honest patient communication. That may not make a thrilling movie scene, but it is exactly how modern medicine should work.
Conclusion
Radio controlled pacemakers are not toys, and they are not helpless gadgets waiting for the nearest hacker. They are sophisticated medical devices that save lives while operating inside an increasingly connected health care system. Past vulnerabilities in RF-enabled cardiac devices show that cybersecurity risks are real. They also show that coordinated updates, regulatory oversight, manufacturer responsibility, and clinician guidance can reduce those risks without sacrificing the benefits of remote monitoring.
The smartest takeaway is simple: do not panic, do not ignore the issue, and do not treat cybersecurity as separate from patient safety. For patients, the right response is to stay connected with the care team and follow official device guidance. For hospitals and manufacturers, the responsibility is bigger: design securely, update responsibly, communicate clearly, and remember that behind every device ID is a person who simply wants their heart to keep doing its job.