Table of Contents >> Show >> Hide
- Quick refresher: What COPD does to the lungs (and why pictures matter)
- Types of pictures used to visualize COPD
- “Normal” lungs vs. COPD lungs: what pictures tend to show
- What COPD can look like on a chest X-ray
- What COPD can look like on a CT scan
- What pictures can’t tell you (and why spirometry still rules)
- Reading a radiology report without spiraling
- Why COPD pictures look different from person to person
- Specific examples: what a “COPD picture” might show in real life
- How to use COPD pictures in a helpful (not scary) way
- Prevention and management: what pictures can motivate you to do next
- FAQ: Pictures of COPD’s effect on the lungs
- Experiences: What it’s like to see COPD in pictures (and live with what they show)
If lungs had a “before-and-after” album, COPD (chronic obstructive pulmonary disease) would be the chapter where the airways get cranky, the air sacs get fragile, and
exhaling becomes way harder than it should be. The tricky part? COPD doesn’t always look dramatic early onso the “pictures” that show COPD’s effect on the lungs
can range from subtle clues to unmistakable changes.
This guide breaks down what different medical images (X-rays, CT scans, and more) can reveal about COPD, what those findings actually mean, and how to talk about your
images with a clinician without feeling like you need a second degree in radiology. We’ll keep it accurate, practical, andbecause breathing is serious but life is still life
occasionally a little funny.
Quick refresher: What COPD does to the lungs (and why pictures matter)
COPD is an umbrella term most often involving emphysema (damage to the air sacs, called alveoli) and/or chronic bronchitis
(long-term inflammation and mucus in the airways). Both can narrow airflow and make it harder to move air out. Think “sticky, narrow pipes” plus “bubble wrap that popped.”
Pictures help because COPD affects lung structureairways, air sacs, and how much air gets trapped. But here’s the big reality check:
images don’t measure how well you breathe. That’s why spirometry (a breathing test) is central for diagnosis and staging. Imaging is the helpful sidekick:
it supports the story, rules out look-alikes, and shows patterns that can guide treatment.
Types of pictures used to visualize COPD
1) Chest X-ray
Chest X-rays are quick and common. They can show signs that suggest COPDespecially when disease is more advancedbut they can also look surprisingly “normal” in
milder COPD. An X-ray is often used to evaluate symptoms (like chronic cough or shortness of breath) and to check for other causes (pneumonia, heart enlargement,
fluid around the lungs, and more).
2) CT scan (Computed Tomography)
CT is the MVP for “seeing” emphysema and air trapping. CT images are more detailed than X-rays and can show:
areas of low density (less tissue, more air), enlarged air spaces, bullae (large air pockets), and signs of small-airway disease.
CT can also help assess distributionupper vs. lower lungsand guide specialized procedures in selected patients.
3) Expiratory CT (breathing out during the scan)
If COPD were a magician, one of its favorite tricks would be air trapping: air gets in, but doesn’t get out efficiently. Expiratory CT is designed to catch that trick
on camera by scanning while you exhale.
4) Pulmonary function test graphics (spirometry printouts)
These aren’t “pictures of the lungs” like scans, but they’re still visual proof of airflow obstruction. The flow-volume loop and the FEV1/FVC ratio tell a story images can’t:
how blocked the airflow is and how much it changes with medication.
“Normal” lungs vs. COPD lungs: what pictures tend to show
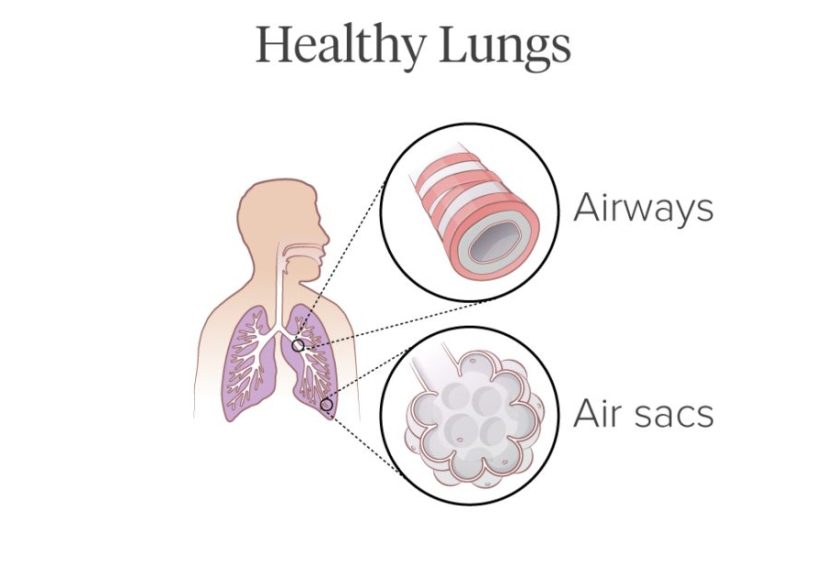
In a healthy lung, alveoli are like tiny, springy clusterslots of surface area for oxygen exchange. In emphysema, the walls between many alveoli are damaged, and smaller
air spaces can merge into larger ones. That means less surface area, less elastic recoil, and more trouble pushing air out.
In chronic bronchitis (one COPD pattern), the airways can look thicker and more inflamed, and mucus can contribute to blockage. On imaging, the differences can be subtle,
and many people have overlapping features.
What COPD can look like on a chest X-ray
An X-ray is like a black-and-white snapshot with limited depth. It won’t show every airway problem, but it can reveal classic “big picture” changes of hyperinflation
(overexpansion due to trapped air) in more advanced COPD.
Common X-ray clues that suggest COPD
- Hyperinflated lungs: the lungs may look larger than expected, sometimes with more visible ribs.
- Flattened diaphragm: instead of a nice dome shape, the diaphragm can look lower and flatter because the lungs stay overexpanded.
- Increased “airiness” (radiolucency): emphysematous areas can look darker because there’s less tissue and more trapped air.
- Bullae (large air pockets): sometimes visible as abnormal air spaces, especially in severe emphysema.
- Smaller-looking heart silhouette: hyperinflated lungs can make the heart look narrower or “compressed” in appearance.
Important nuance: a chest X-ray can support a COPD picture, but it usually can’t confirm COPD on its own. Many clinicians use it as a starting point and to rule out other
problems that can mimic COPD symptoms.
What COPD can look like on a CT scan
CT is where COPD becomes more “visible,” especially emphysema. On CT, emphysema can appear as low-attenuation areas (regions that look darker because
they contain less lung tissue). CT can also show airway changes and air trapping patterns that don’t reliably appear on a plain X-ray.
Emphysema patterns you might hear about
Radiologists sometimes describe emphysema by distribution. You don’t need to memorize these, but recognizing the words can help you decode a report:
- Centrilobular emphysema: commonly linked with smoking; often more prominent in upper lungs.
- Paraseptal emphysema: near the edges of the lung; sometimes associated with blebs/bullae.
- Panlobular emphysema: can be associated with alpha-1 antitrypsin deficiency and may affect lower lungs more.
Bullae: when air pockets get “too big to ignore”
A bulla is basically an oversized air space formed when normal lung tissue is destroyed and replaced by a large pocket of air. On CT, bullae can look like
very dark, sharply defined spaces. Small bullae may just be noted, while very large ones can compress healthier lung around them, affecting breathing more.
Air trapping: the COPD “receipt” you can see on expiratory CT
If you’ve ever tried to empty a balloon with a tiny straw, you get the idea. With COPD, narrowed airways make it hard to exhale fully before the next breath begins.
Expiratory CT may show areas that stay abnormally “air-filled” after exhalationevidence of gas trapping.
This matters because air trapping contributes to hyperinflation, which can make the diaphragm less effective. When the diaphragm flattens and loses its
natural curve, breathing can feel like you’re doing extra work for the same amount of air. (Not exactly the kind of workout anyone asked for.)
What pictures can’t tell you (and why spirometry still rules)
Images can show structural changes, but they don’t directly measure airflow limitationespecially early on. Two people can have CT-visible emphysema and feel very different,
and the opposite can happen too: someone can have significant symptoms with relatively subtle imaging findings.
That’s why clinicians typically rely on spirometry to confirm COPD. Spirometry looks at how much air you can exhale in one second (FEV1) and the total amount exhaled (FVC),
and it uses the ratio (FEV1/FVC) to identify airflow obstruction. Imaging then helps provide context and can identify related issues or alternative diagnoses.
Reading a radiology report without spiraling
Radiology reports can feel like they were written by someone paid per syllable. Here are common phrases that show up in COPD imaging reports and what they usually mean in plain
English:
- “Hyperinflation” / “hyperexpanded lungs”: signs of trapped air and overexpanded lungs.
- “Flattened diaphragms”: often linked to hyperinflation; the diaphragm sits lower and looks less dome-shaped.
- “Emphysematous changes”: CT-visible areas where alveolar damage has reduced normal lung tissue.
- “Bullous disease”: presence of bullae (large air pockets).
- “Bronchial wall thickening”: can be associated with chronic airway inflammation (seen in chronic bronchitis and other conditions too).
- “Air trapping on expiratory images”: suggests small-airway obstruction; air isn’t leaving evenly when you exhale.
Pro tip: if you’re reading your report and your brain starts doing worst-case-scenario parkour, pause and jot down questions for your clinician. “How severe is this?”
and “What does this mean for my day-to-day breathing?” are often more useful than trying to self-diagnose from imaging words alone.
Why COPD pictures look different from person to person
COPD isn’t one single “look.” Images vary depending on:
- Type of COPD pattern: emphysema-predominant vs. chronic bronchitis-predominant vs. mixed.
- Severity: mild COPD may show minimal imaging changes.
- Distribution: upper-lobe vs. lower-lobe predominance can differ by cause and subtype.
- Triggers and exposures: smoking, secondhand smoke, occupational dust/fumes, air pollution, and genetics can all contribute.
- Technique: how deep the breath was during imaging and whether expiratory views were done can affect what’s visible.
Specific examples: what a “COPD picture” might show in real life
Example 1: The chest X-ray that hints at COPD
A person with long-term shortness of breath gets an X-ray. The report notes “hyperinflated lungs” and “flattened hemidiaphragms.” No pneumonia is seen. This doesn’t
diagnose COPD by itself, but it supports the clinical suspicionespecially if spirometry shows airflow obstruction.
Example 2: The CT scan that reveals emphysema
Another person gets a CT because symptoms don’t match a normal-ish X-ray. The CT shows scattered low-density areas consistent with emphysema, and a couple of bullae near
the lung edges. This helps confirm that structural lung changes are present and can guide conversations about inhalers, pulmonary rehab, and risk reduction.
Example 3: Expiratory CT that explains “I can’t get the air out”
Someone says, “Inhaling is hard, but exhaling is worse.” An expiratory CT shows patchy air trappingareas that don’t empty properly on exhalation. That image can help
explain symptoms and may influence treatment planning.
How to use COPD pictures in a helpful (not scary) way
Medical images can be empoweringespecially when you use them as a conversation tool instead of a doom scroll.
Questions worth asking at your next appointment
- What findings on my imaging suggest COPD, and how confident are we?
- Do my images look more like emphysema, chronic bronchitis, or both?
- Is there evidence of bullae or significant hyperinflation?
- Do I need spirometry (or repeat spirometry) to confirm or monitor?
- Are there other conditions the images suggest we should rule out?
If you have access to your images, ask your clinician to point out one or two key features on-screen. Even a two-minute walkthrough can turn a confusing black-and-white
picture into something that makes sense.
Prevention and management: what pictures can motivate you to do next
COPD has no cure, but there’s a lot you can do to slow progression and improve quality of life. Seeing structural changes on imaging can feel like a wake-up callbut it can
also be a roadmap.
- Reduce exposures: avoiding tobacco smoke (including secondhand smoke) is huge; workplace and environmental exposures also matter.
- Get the right testing: spirometry helps confirm diagnosis and track changes.
- Use treatments consistently: inhalers, pulmonary rehab, vaccines, and action plans for flare-ups can reduce symptoms and exacerbations.
- Ask about genetics when relevant: if COPD shows up unusually early or without major smoking history, alpha-1 antitrypsin deficiency testing may be considered.
FAQ: Pictures of COPD’s effect on the lungs
Can a chest X-ray diagnose COPD?
A chest X-ray can show signs that suggest COPD (like hyperinflation or flattened diaphragms), but it usually can’t confirm COPD by itselfespecially in milder disease.
Spirometry is typically used to confirm airflow obstruction.
Is CT always needed to see COPD?
Not always. Many people are diagnosed with spirometry and clinical history. CT is especially helpful when the diagnosis is uncertain, symptoms don’t match other results, or
when clinicians need more detail about emphysema distribution, bullae, or other lung problems.
Why do my symptoms feel worse than my pictures look?
COPD symptoms reflect airflow, inflammation, fitness level, and other health factorsnot just what’s visible on an image. Small-airway disease can cause major symptoms even
when large structural changes aren’t obvious.
What does “hyperinflated lungs” mean on a report?
It generally means the lungs are holding extra airoften because narrowed airways make it hard to exhale fully. Hyperinflation can flatten the diaphragm and make breathing
feel more work-intensive.
Experiences: What it’s like to see COPD in pictures (and live with what they show)
Medical images can feel oddly personal. They’re not selfies, but they can still hit like oneespecially when a radiologist points at your lungs and says something that sounds
both clinical and life-altering. People who go through COPD workups often describe a mix of emotions: relief at getting an explanation, frustration that it took so long,
and a sudden urge to learn a new language called “radiology report.”
One common experience is the “wait…that’s my diaphragm?” moment. A clinician might show a chest X-ray and explain that the diaphragm looks flatter than expected because the
lungs are staying too inflated. For many people, that visual connects dots that words never did. Shortness of breath stops feeling like a vague complaint and starts looking
like something with a physical footprint. And while that can be scary, it can also be validating: “I’m not lazy. I’m not imagining it. My lungs are doing extra work.”
CT scans often bring a second wave of reactionsbecause CT is more detailed and the findings can sound dramatic. “Low attenuation,” “bullae,” “emphysematous changes”:
those phrases can feel like the lungs have been graded on a curve you didn’t study for. Many people say the most helpful part is when a clinician translates it into
practical meaning: which parts of the lungs are affected, whether there’s significant air trapping, and what can realistically improve symptoms (like inhalers and pulmonary
rehab) versus what’s about slowing progression (like avoiding smoke and irritants).
Another shared experience is learning that pictures are only part of the story. Some people have CT-visible emphysema and still walk daily with manageable symptoms; others
have fewer obvious imaging changes but feel breathless climbing a single flight of stairs. That mismatch can be confusing until spirometry enters the chat. Seeing a
flow-volume loop or a reduced FEV1/FVC ratio can be the “aha” moment: it shows the airflow problem in a way that complements the structural pictures.
People also talk about how images can change motivation. A CT scan that clearly shows emphysema can make quitting smoking feel less like a lecture and more like a
time-sensitive decision. For those who never smoked, learning about workplace exposures or genetic risks (like alpha-1 antitrypsin deficiency) can bring a different kind of
determination: advocating for testing, improving air quality, or taking symptoms seriously instead of brushing them off as “just getting older.”
Over time, many people describe a shift from fear to strategy. The images become less of a verdict and more of a baseline. “This is where we’re starting.” Follow-up visits
focus on action plans: recognizing flare-ups early, staying consistent with meds, doing pulmonary rehab exercises, and protecting the lungs from infections. And yes, there’s
often some dark humorbecause if you can’t laugh a little while learning terms like “hyperinflation,” you might scream instead. (Not recommended. Screaming is cardio,
and cardio is rude when your lungs are already busy.)
If you’re reading this because you’ve seen COPD mentioned in your imaging or you’re searching for pictures of COPD’s effect on the lungs, here’s the most grounded takeaway:
you’re allowed to feel a lot about itand you’re also allowed to ask for clarity. Ask someone to show you the findings. Ask how they connect to your symptoms. Ask what you
can do next. Pictures can be powerful, but the goal isn’t to stare at them forever. The goal is to use them to breathe a little easier in real life.